Suppose a pharmaceutical company has developed a new drug for lowering blood pressure, and they are preparing a clinical trial (experiment) to test the drug’s effectiveness. They recruit people who are taking a particular standard blood pressure medication. People in the control group will continue to take their current medication through generic-looking pills to ensure blinding. Write down the hypotheses for a two-sided hypothesis test in this context.
Solution.
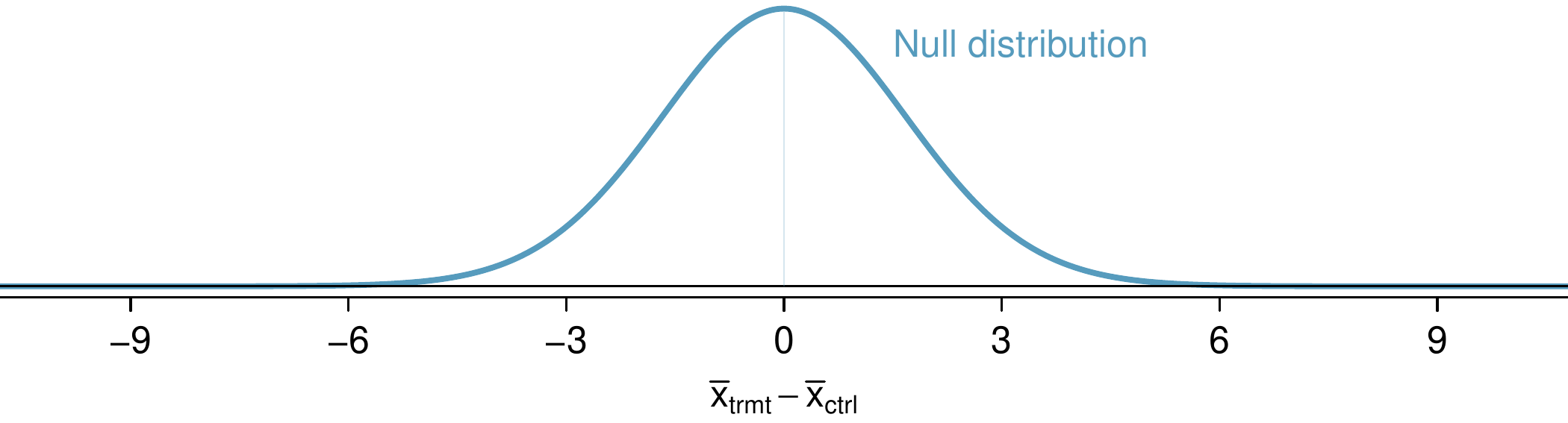
Generally, clinical trials use a two-sided alternative hypothesis, so below are suitable hypotheses for this context:
- \(H_0\text{:}\)
-
The new drug performs exactly as well as the standard medication. \(\mu_{trmt} - \mu_{ctrl} = 0\text{.}\)
- \(H_A\text{:}\)
-
The new drug’s performance differs from the standard medication. \(\mu_{trmt} - \mu_{ctrl} \neq 0\text{.}\)